In recent times our staff has been flooded with inquiries about the Epistane from Labolic. Does it work? How it works? Does it blocks our HPTA? What to take? What to take it with? or how does it interact with drugs or alcohol? And in fact finding those information can be a problem for a relatively short time of occurrence of it on market and complicated mechanism of action which effectively discourages the "dietetic portals" to address the topic. To meet expectations we decided to sum up all available knowledge about Epistane - the active ingredient of this product.
- Epistane - what is it?
- What can we say for sure about the effect of methylation
- What can we suppose based on the analogy of other methylated compounds?
- How does Epistane work?
- PCT? Liver support on cycle? Health hazards?
- Exemplary PCT cycle after Epistane
- What to combine Epistane with?
- The remaining "company" depends on the goals we want to achieve.
- Summary
- References:

Epistane - what is it?
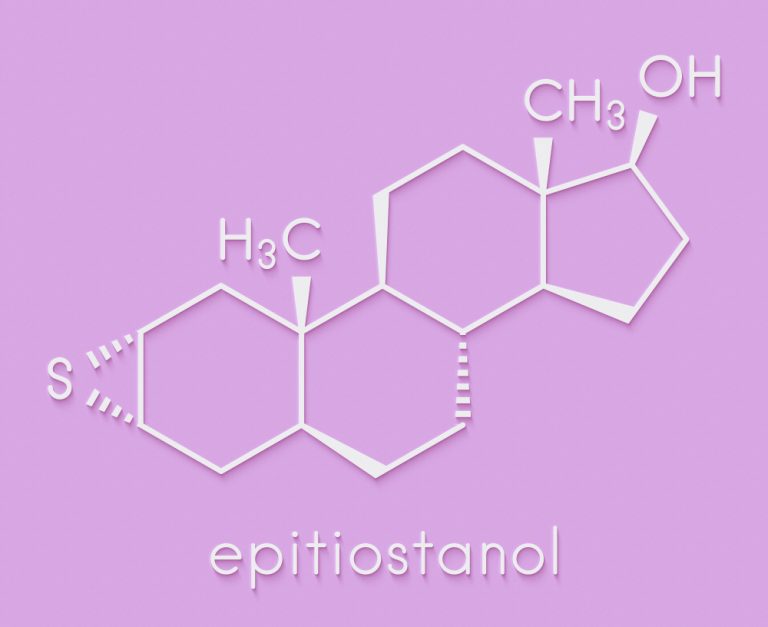
Epistane (actually 2a, 3a-epithio-17a-methyl-17b-hydroxy-5a-adrostan) is a methylated derivative of Epitiostanol (Thiodrol). Epitiostanol is used as an estrogen-lowering agent as well as an anabolic-androgenic steroid in injections.
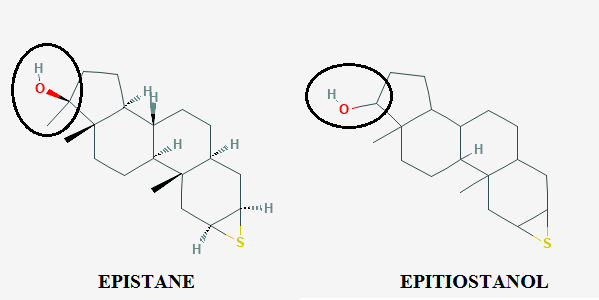
The key here is the additional methyl group at position 17a.
(for ease of reference place of 17th carbon was marked)
Probably the question "What does one line change in a whole compound" appears. In the simplest terms - it allows you to effectively use the agent in oral intake
What can we say for sure about the effect of methylation
Methylation prevents the deactivation of the compound by the first-pass effect (this effect drastically reduces the concentration of the substance before it actually appears in the blood circulation). Methyl group at 17a position protects the hydroxyl group at 17b position from oxidation which would normally deactivate most of the active substance. This increases the bioavailability of the compound so much that there is a sense of its use orally (in the absence of methylation the effective dose of the compound would be much higher which would result in much higher costs of cycle and higher liver toxicity)
What can we suppose based on the analogy of other methylated compounds?
We can say with great certainty that methylation increases the additional androgenic and anabolic affinity by analogy.
For example, we can take trenbolone and its methylated version. While the effective dose of the first one is several milligrams (30-50mg / injections ed or eod but this is a highly individual issue) the effective dose of its methylated derivative clarifies at a level never exceeding 1 milligram! A similar relationship can also be noticed between progestins and their alkylated * derivatives
The significant issue however is that this effect is relatively poorly studied and in research usually occurs as an annotation or accidental discovery of the intensification of the compound's activity. It is also not possible to transfer this effect with certainty to the comparison of Epistane-Epitiostanol by the lack of specific studies comparing these two agents. However, a repetitive pattern implies that alkylation actually enhances androgenic affinity
* -alkylation is the process of attaching hydrocarbon groups. Methylation is the most common of these (addition of the methyl group -CH3) however alkylation with longer hydrocarbons also occurs hence a more general term is used
How does Epistane work?
It is vain to look for research relating directly and strictly to Epistane's activity. The closest therefore will be based on the effect of Epitiostanol and the effects resulting from the modification of the structure described above.
It can therefore be concluded that Epistane binds to the androgen and estrogen receptors being an agonist of the former and an antagonist of the latter.
Agonism to androgen receptors is the basis of action here. This results in increased expression of male traits - in our case the most important is the increase in muscle protein synthesis (through indirect activation of IGF-1R receptors and their sensitization to IGF). In addition pro-androgen affinity prevents excessive fat deposition by blocking the signaling pathway normally supporting the differentiation of fat cells.
Antagonism to estrogen receptors eliminates the biological effects of estrogen which translates into a reduction in the risk of gynecomastia as well as impaired expression of male sex characteristics.
PCT? Liver support on cycle? Health hazards?
The common opinion is that "if you do not have to do the Epi retaliation it means it was not Epi." Despite the pejorative overtone there is a lot of truth in this sentence. Epistane is an anabolic-androgenic steroid; a derivative of dihydrotestosterone which at the same time indicates its very good effectiveness as well as the health consequences resulting from it.
First of all - for the anti-estrogen properties with increased caution should be approached people with a naturally high level of SHBG (sex hormone binding globulin) proteins because they are more likely to the phenomenon of gynecomastia.
Technically the risk of gynecomastia may arise by the possibility of conversion of Epistane to DHT (which may result in excessive hair loss acne or aggression) but this risk should only be considered in stacks (Epistane stacking with other 17-alfa-methylated agents is not recommended) However apart from both of the above cases Epistane acts anti-estrogen'ish and can be used as a suppressant of gynecomastia.
More common side effects are prostatic hyperplasia and deterioration of the lipidogram. Due to the antiestrogenic effect it can also adversely affect the joints and cause stiffnes.
Another effect of Epistane is the reduction of appetite and increased fatigue. It is usually associated with the fact that all 17-alpha-methylated agents are exceptional stressors to the liver therefore highly recommended (even required) protective measures should be taken during the cycle especially in case of any liver hypersensitivity (however it should be noted that Epistane is not considered a very burdening agent of the liver however it does not change the fact that it is necessary to take care of the liver during the cycle - hepatic tests during the cycle should also be indicated)
Each anabolic steroid has an impact on the HPTA axis to a greater or lesser extent. This is a key statement from which we must start a discussion on the issue of prudence.
People who do not have to do PCT are isolated cases and they mainly belong to people who are more often on the cycle than they are not (using PCT then causes huge "Rollercoaster" for the endocrine system which is not advisable) and people with naturally low testosterone (PCT supports the production of natural testosterone so it is practically senseless in this case - such people are recommended to return to post-cycle testosterone replacement). It should be noted that the appropriate PCT should be selected after completing the test after cycle (LH, FSH + testosterone) and on the basis of nonconformities that are indicated in them.
However in order to give some specific information the practice in the case of Epistane indicates that excessive estrogen production after the cycle seems to be the main problem. Epistane acts anti-estrogen'ish so stopping the cycle can cause excessive estrogen production which can lead to gynecomastia and problems with erection. PCT does not have to be excessively complicated and is most often based on the use of a single SERM (selective estrogen receptor modulator (Tamoxifen / Clomid)) at a dose selected by post-cycle tests results cycle length and dosages used during the cycle.
Exemplary PCT cycle after Epistane
Cycle - 5 weeks Epistane 30/40/40/40/50
Nolvadex - 4 weeks 20/20/10/10
Clomid - 4 weeks 50/50/25/25
What to combine Epistane with?
The basic companion for the use of Epistane should be liver support agents. Preparations based on TUDCA (tauroursodeoxycholic acid) should be sufficient. The first measure recommended for Epistane is also often testosterone however, we are aware that using oral means one of the main reasons is to avoid injection.
An interesting complement to the cycle is also Laxogenin which unless in itself is not the most effective substance fantastically complements the "heavier" gear during the cycle supporting anabolic effects and contributing to maintaining a higher energy level and lipolysis (by increasing the level of circulating in the body of cAMP).
A good supplement will also be a good preworkout booster. Epistane itself does not affect the increase of arousal and the appropriate stimulation will allow you to maximize the benefits of a more optimal hormone level during the cycle.
The remaining "company" depends on the goals we want to achieve.
If we use Epistane in the reduction cycle (strength optimization, recomposition) addition of yohimbine and GW-501516 will be a great choice. Yohimbine is one of the few really effective measures to support reduction so you can always find a place for it to focus on reducing your body fat (you han check our earlier article about it if you are interested).
Read more: How does Yohimbine HCl works?
GW-501516 (Cardradine) for this will additionally support the reduction of adipose tissue by affinity to PPAR-beta receptors. This action is identical for the body to the stimuli experienced during the feeling of hunger which forces the intensified use of spare body fat.
With the desire to increase strength or muscle mass, an interesting idea may be an addition of MK-677 (Ibutamoren). One of its main activities - blocking the activity of somatostatin (growth hormone binding protein) - allow for even greater abolition of natural limits of muscular tissue procurement by more comprehensive influence on the "bias" of the hormonal economy.
Summary
Epistane is not a playtoy. It should be used with extreme caution and treated as a full-fledged anabolic steroid
This involves the need to use protective measures perform tests and establish correct PCT on their basis. However thanks to this we also have a measure with great potential for both reduction and mass building cycles. Epistane is not another agent that works in the background works on a placebo principle or works selectively. It is an effective anabolic-androgenic steroid.
And it seems that the best culmination of the topic will be a well-known quote from the Spider-Man universe - "With great power comes great responsibility"
References:




